
Low risk early stage cancer
The benefit of radiation is mostly local control in the treated breast. In a woman over the age of 65, the chance of an early stage estrogen-responsive cancer <3cm in size (that has not gone to the lymph nodes) recurring in the same breast is about 0.5-1% per year after lumpectomy if she remains on a hormone blocker for 5 years. If a woman lives longer than 10-15 years after her treatment, then we could see a 5-15% chance of the cancer recurring in that breast. Radiation over 5 or 15 days could reduce that 10-15 year risk to <2%.
Thus, when making a decision whether to forego radiation after lumpectomy, my personal bias is to “buy the extra insurance” so that the cancer won’t come back in the patient’s lifetime if she is younger or relatively healthy. Often, these women are good candidates for partial breast radiation over one week with minimal expected side effects.
Distant recurrence
Unfortunately, even in the lowest risk breast cancers, the chance that it shows up in other parts of the body are not insignificant. For cancers that respond to a hormone blocker, taking these daily pills to reduce estrogen in the body can reduce the relative risk of dying from breast cancer by 1/3, or about a 10% absolute risk reduction.
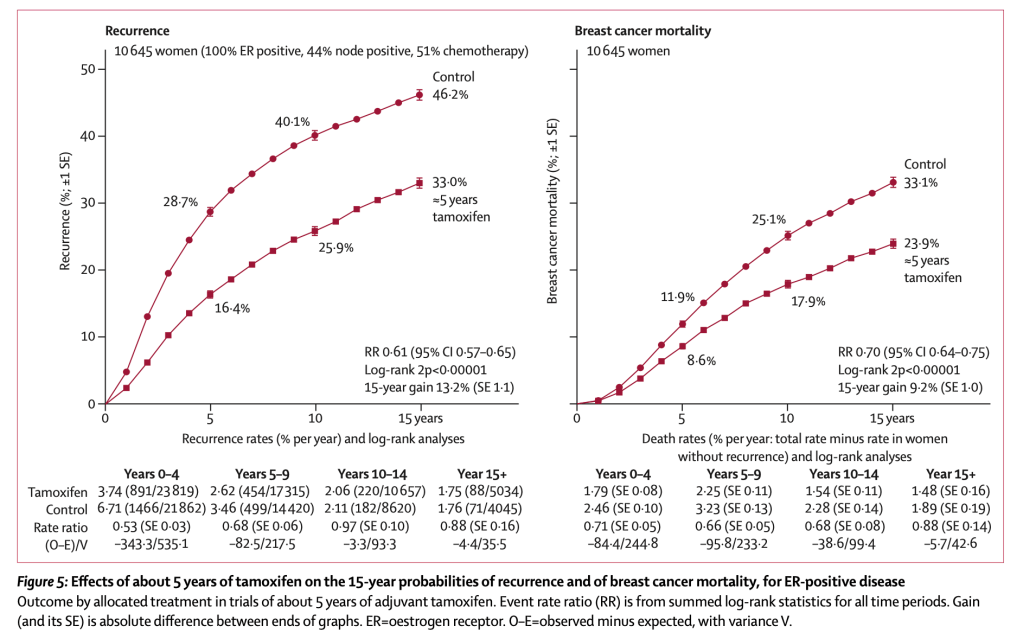
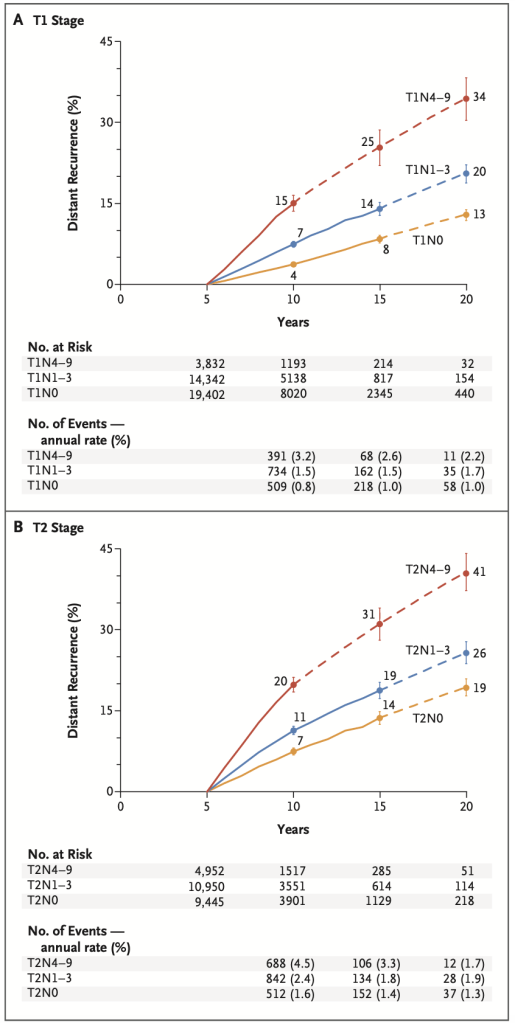
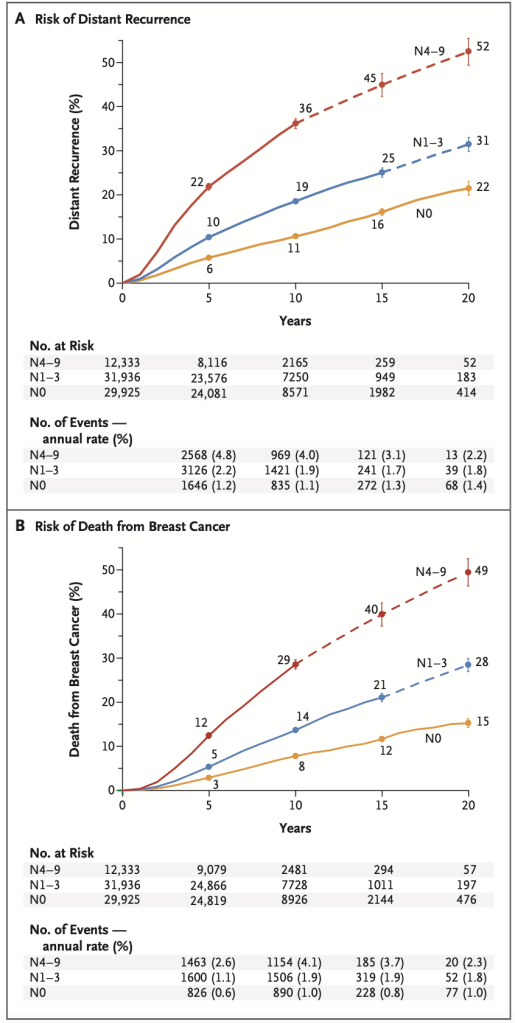
Even after taking the hormone blockers for 5 years, the risk of distant spread and death never goes away. This follow up meta-analysis has several useful charts.
In addition to chemotherapy, pre-menopausal women may benefit from more intense hormone blockade. There are new systemic treatments such as PARP inhibitors, HER2-specific therapies, immunotherapy for triple negative disease, and targeted therapies that are improving these distant spread numbers, but I’m wandering out of my area of expertise and rely on my medical oncologist colleagues for further discussions of these rapidly advancing trials.
